Spatial Analysis and Modelling of Malaria Trend in Si Sa
Ket Province, Thailand
Noradee, S.,1,2Uthaipibull, C., 3 Kanjaras, P.
1,2 and Nithikathkul, C. 1,2*
1Ph.D in Health Science Program, Faculty of Medicine,
Mahasarakham University, Mahasarakham, Thailand

2Tropical Health Innovation Research Unit, Faculty of
Medicine, Mahasarakham University, Thailand
3Thailand Center of Excellence for Life Sciences (Public
Organization), Thailand
*Corresponding Author
Abstract
Malaria is a public health problem in tropical regions. The
Regional Health office has a program to educate residents about
what malaria disease is, how to reduce malaria infection and who
have no immunity or little to malaria, such as young children and
pregnant women or even who have knowledge about malaria. The
overall Si Sa Ket malaria prevalence was still high in the Khun Han
district, with P. vivax at 74.0 % and P. falciparum at 24.5%. Most
of them were agricultural and aged around 16 – 45 years. A factor
related to severe malaria in Si Sa Ket province was that infection
in males was 2.49x more than in females (95% Confidence interval
(CI) = 1.11-2.45), Military personnel were 2.93x more likely to be
infected than in other occupations (95%CI = 1.45 - 6.57) and mixed
of Plasmodium species infection about 3.34x more than other
Plasmodium species (95%CI= 0.31 - 0.73). The outcome of this study
can be applied to the malaria surveillance system cooperatively
achieved by the Vector-borne Disease Control Project with the
Ministry of Public Health of Thailand when comparing infection rates
reported in similar studies. In addition, the results of this study
indicate overall that the efforts of the Department of Health are
going well. The low rate of sick individuals shows that the
residents received enough information to get an infection of
malaria. This report intends to provide beneficial information to
the inhabitants and locals of Si Sa Ket Province Health Department
to improve other malaria-prevention programs.
Keywords: Geographic Information System, Plasmodium spp., Severe Malaria, Vector Index
1. Introduction
In the global environment of both local and global change scenarios,
the physical phenomena and health informatics issues are changing from
personal to global. Health records about tropical disease outbreaks and
non-communicable diseases among all the national and international
health organisations still require new technology approaches to create
prevention and control care and integrate multidiscipline networks
[1]
[2]
[3]
[4]
[5]
[6]
[7]
[8] and [9]. Malaria remains a dangerous
disease that affects human health. As well known, malaria was born by
Anopheles mosquitoes that are infected by Plasmodium
parasitic protozoa (P). Only five Plasmodium protozoa
are infected in humans, Plasmodium falciparum,
Plasmodium vivax, Plasmodium malariae, Plasmodium ovale and
Plasmodium knowlesi [10]. This disease can be founded in tropical regions and also in most
of South and Central America, Africa, the Middle East, and the Indian
subcontinent, southeast Asia and Oceania [11]. Most malaria symptoms
are fever and headache because of parasite invasion of red blood cells
[10]. In 2018, almost 228 million malaria cases were certified
globally, of which 93% were found in Africa, followed by southeast Asia
and the eastern Mediterranean regions [12]. In addition, malaria
continues to be a critical problem in the world, especially in the
Greater Mekong Sub-region (GMS) [13]. The GMS are Cambodia, Yunnan
province and Guangxi Zhuang autonomous region, The Lao People’s
Democratic Republic, Myanmar, Thailand, and Viet Nam [13]. According to
the GMS annual malaria report, between 2012 to 2017, malaria cases have
been steadily decreasing, including mortality rates from malaria during
the same period. On the other hand, artemisinin resistance has been
demonstrated in many spaces of the Great Mekong sub-region in the past
decade.
That indicates treatment failure rates occurring in the Great Mekong
sub-region. Not only resistance to artemisinin but also resistance to
artemisinin-based. combinations were also observed [13]. Once more,
resistance to artemisinin-based combination therapies (ACT) has
increased in many countries of GMS [14] and [15]. A policy for malaria
eradication in the GMS was to eliminate malaria in GMS countries within
2030. Specifically, the critical activities required to fight malarial
drug resistance in the region eliminating Plasmodium falciparum
in 2025 [14]. All countries with decreased malaria burden by operating
to elimination. When they have an entire rate of less than 1 case per
one thousand people yearly, that is World Health Organization (WHO)
guidelines [13]. Thailand has established a strategy to eradicate
malaria using Thailand's National Malaria Elimination Strategy
(2017–2026), including increasing the zero malaria zone to 100% by 2023
[16]. Malaria incidence in Thailand, the Department of Disease Control
(DDC) reports that malaria has steadily decreased over the past five
years [12]. The distribution of malaria appears to be mainly around the
border area, such as Thailand – Myanmar border and Thailand – Cambodia
border. Moreover, the World Health Organization expressed concern over
the evolution of artemisinin-resistant P. falciparum parasites
along the Cambodia-Thailand border, Especially in Si Sa Ket and Ubon
Ratchathani [14]. We found many studies which indicate that the
prevalence of malaria is affected by environmental factors such as
temperature that affects the biological clock of malaria, the parasite
cannot grow below 18°C and over 40°C [17] and [18], altitude affects
temperature variation through a 200 meter increase in height; the
temperature declines every one °C. Therefore, elevation can indirectly
affect the prevalence of malaria because of its effect on temperature
[19]. Water bodies are a significant factor influencing malaria
prevalence and case scenarios. Water bodies are fundamental as larval
breeding locations for anopheles [20]. This is the first
report on malaria phenomena with climate changes and the factors
relevant to malaria prevalence in Si Sa Ket province using a geographic
information system (GIS) to look for trends in the disease's status and
guidelines used to prevent an epidemic. The crucial outcome showed the
integration of situations by defining a malaria burden and creating a
malaria map in Si Sa Ket Province, Thailand.
2. Material and Methods
This phenomenal malaria prevalence observation by the General
Communicable Disease Control Division, Si Sa Ket Provincial Health
Office, Si Sa Ket Province, Thailand with the outbreak and
environmental factors affecting malaria’s prevalence in Si Sa Ket
province, Thailand. We combined the malaria cases from government
healthcare facilities in Thailand between 2015 and 2020.
2.1 Data Source
2.1.1 Study area
The study area was Si Sa Ket in northeastern Thailand (Figure 2). Si Sa
Ket’s population are estimated to be 1,458,324 [21]. The site is 22,895
km2. Si Sa Ket is warm, with an average temperature of 26.8
°C and precipitation of about 1242 mm [22]. Si Sa Ket borders a part of
Cambodia. Most of them are engaged in agricultural production.
2.1.2 Malaria Data
A malaria patient was diagnosed by health personnel or a malaria
volunteer trained in a malaria treatment procedure [23]. According to
the Department of Disease Control, confirmed malaria cases that tested
positive specific results for
Plasmodium falciparum, Plasmodium vivax
, or both (“Mixed”) rapid diagnosis test kits (RDT) were used for
active surveillance. Microscopics were used when an RDT had a positive
result [24]. Moreover, Malaria parasites can be identified by
microscopic. That is the gold standard for malaria diagnosis [24].
Malaria case data were collected from the Active surveillance system,
the General Communicable Disease Control Division, Si Sa Ket Provincial
Health Office, Si Sa Ket Province, Thailand, for six years (2015 to
2020). Moreover, data concerning Thailand’s malaria prevalence was
collected from the Thailand malaria elimination program, Department of
Disease Control, Ministry of Public Health, Thailand, from 2015 to
2020. All the data were collected from an online database.
2.1.3 Population density and mapping
Population data were collected from the Department of provincial
administrators, ministry of Interior, available from 2015 to 2020 [21].
The Thailand map and Si Sa Ket province boundary map were obtained from
http://www.DIVA-GIS.org [25]. Population data and maps were collected
from an online database.
2.1.4 Environmental variables
In this study, two types of environmental data were used. Dynamic
variables included ecological conditions expected to vary in this
study. The author collected only two variables, average land surface
temperature and average rainfall. Ecological data were received from
Thailand’s Meteorological Department and http://www.ClimateData.org
from 2015 to 2020 [22] and [26], and fifteen field meteorological
stations in Si Sa Ket province were collected. Static variables
included variables related to geography and physiography that were not
expected to vary from year to year. In this study, only an altitude was
used. The altitude map was collected from http://www.DIVA-GIS.org [25].
2.2 Data Analyse
2.2.1 Socio-demographic, prevalence and severe risk factors
Statistical analysis used frequencies and percentages to describe
malaria distribution. Malaria prevalence rates were determined (as the
number of cases per 1,000 people yearly) for Thai and foreigners in Si
Sa Ket province. This study aims to explain factors related to severe
malaria. Multivariable logistic regression was used. First, fisher’s
exact test was used to show the relationships between factors and
severe malaria. Then, univariable logistic regression was used to
explore factors affecting severe malaria. Univariable analysis was
performed using odds ratio (OR) and 95% confidence intervals (CI).
Next, we took variables with results P-value<0.25 into the last
multivariable analysis model. A step-backwards elimination technique
was used to describe a robust model from the initial to the last model.
The variables that remained significant (P-value<0.05) were kept in
the model, using adjusted odds ratio (AOR) and 95% confidence intervals
(95%CI) were also calculated. STATA version 17 was used for this
analysis.
2.2.2 Spatial data
The data was modified to create geographic information using ArcGIS
10.5. meteorological data, including average rainfall data and average
temperature from ClimateData.org and The Meteorological Department of
Thailand from 2015 to 2020 [22] and [26], were used to explore the
distribution of malaria and factors related to the malaria epidemic in
Si Sa Ket Province.
The research assistant was trained to collect the coordinates position
of malaria patients in study areas. They have used interpolation
analysis, especially inverse distance weight (IDW), to illustrate
malaria prevalence and average rainfall in study areas. Fifteen field
meteorological stations were used for interpolation analysis. An
overlay technique was performed to represent a relationship between
population density and malaria prevalence. Moreover, correlation
analysis explored factors such as average land surface temperature
influencing malaria prevalence. The altitude map was collected from
http://www.DIVA-GIS.org [25]. The elevation map described the
relationship between malaria prevalence and altitude.
3. Result
3.1 Socio-demographic and Malaria Incidence Rate in Si Sa Ket
Province
1,259 malaria cases were reported to Si Sa Ket’s active surveillance
system, Ministry of Public Health, from 2015 to 2020 (0.47/1000
population) (Table 1). The highest prevalence was presented in 2015,
with 0.95 /1000 population (574 malaria), while in 2020, the lowest
rate was reported, with 0.02 (20 malaria). The overall malaria
prevalence was high in Khun Han district, followed by Phusing and
Kantharalak districts. Most of the patients were in agriculture sector
and lived around the Thai-Cambodia border. Adults aged 16–45 had a
chance of malaria risk among other groups. Most patients were more
infected with P. vivax than P. falciparum. Since
2019, Thailand has replaced malaria medication, a previous study found
that drug efficacy decreased in 2019. Si Sa Ket and Ubon Ratchathani
province used Artesunate – Pyronaridine as the first-line drug.
Therefore, malaria prevalence dropped (Table 1). Figure 1 illustrates
the weekly malaria epidemic curve from 2015 to 2020.
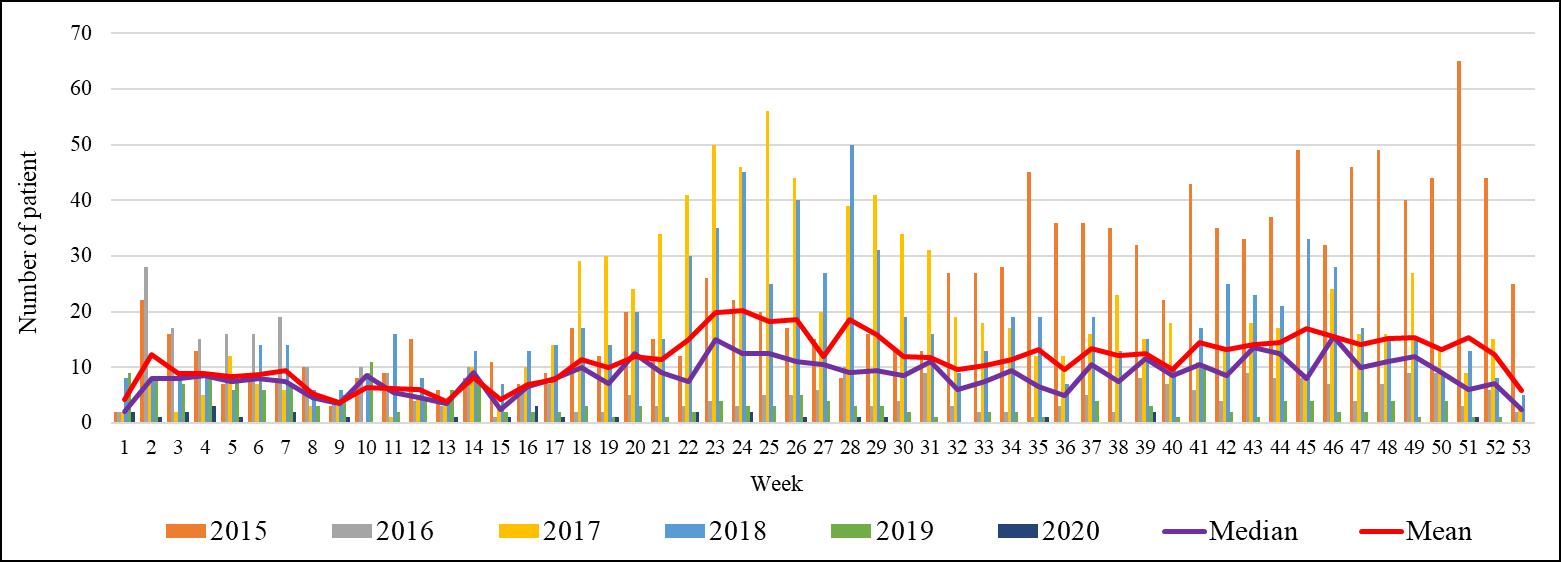
Figure 1: A malaria epidemic curve (weekly report) in
Si Sa Ket Province during 2015 – 2020
Table 1: The prevalence rate (case/1,000 population) of
malaria in Si Sa Ket Province during 2015 - 2020
|
District
|
2015
|
2016
|
2017
|
2018
|
2019
|
2020
|
Avg. PR.
|
|
Mueang Si Sa Ket
|
0.21
|
0.01
|
0.06
|
0.06
|
0.00
|
0.00
|
0.06
|
|
Yang Chum Noi
|
0.13
|
0.00
|
0.00
|
0.07
|
0.00
|
0.00
|
0.03
|
|
Kanthararom
|
0.11
|
0.01
|
0.05
|
0.04
|
0.01
|
0.00
|
0.04
|
|
Kantharalak
|
1.83
|
0.43
|
1.25
|
1.55
|
0.28
|
0.04
|
0.89
|
|
Khukhan
|
0.21
|
0.03
|
0.18
|
0.09
|
0.01
|
0.01
|
0.09
|
|
Phrai Bueng
|
0.29
|
0.03
|
0.08
|
0.40
|
0.03
|
0.00
|
0.14
|
|
Prang Ku
|
0.05
|
0.02
|
0.15
|
0.02
|
0.00
|
0.00
|
0.04
|
|
Khun Han
|
8.01
|
2.59
|
5.80
|
5.95
|
1.33
|
0.14
|
3.96
|
|
Rasi Salai
|
0.04
|
0.01
|
0.00
|
0.00
|
0.00
|
0.00
|
0.01
|
|
Uthumphon Phisai
|
0.04
|
0.01
|
0.02
|
0.02
|
0.00
|
0.01
|
0.02
|
|
Bueng Bun
|
0.00
|
0.00
|
0.22
|
0.00
|
0.00
|
0.00
|
0.04
|
|
Huai Thap Than
|
0.03
|
0.00
|
0.00
|
0.00
|
0.00
|
0.00
|
0.00
|
|
Non Khun
|
0.15
|
0.00
|
0.05
|
0.00
|
0.00
|
0.00
|
0.03
|
|
Si Rattana
|
0.02
|
0.04
|
0.02
|
0.08
|
0.00
|
0.00
|
0.03
|
|
Nam Kliang
|
0.23
|
0.02
|
0.05
|
0.09
|
0.00
|
0.00
|
0.06
|
|
Wang Hin
|
0.03
|
0.03
|
0.00
|
0.00
|
0.00
|
0.00
|
0.01
|
|
Phu Sing
|
4.13
|
1.49
|
4.57
|
2.72
|
0.66
|
0.16
|
2.28
|
|
Mueang Chan
|
0.00
|
0.00
|
0.06
|
0.00
|
0.00
|
0.00
|
0.01
|
|
Benchalak
|
0.08
|
0.00
|
0.22
|
0.08
|
0.03
|
0.03
|
0.07
|
|
Phayu
|
0.12
|
0.06
|
0.03
|
0.00
|
0.00
|
0.00
|
0.04
|
|
Pho Si Suwan
|
0.04
|
0.00
|
0.04
|
0.00
|
0.00
|
0.00
|
0.01
|
|
Sila Lat
|
0.10
|
0.00
|
0.10
|
0.00
|
0.00
|
0.00
|
0.03
|
|
Total
|
0.95
|
0.28
|
0.73
|
0.69
|
0.14
|
0.02
|
0.47
|
Avg. = average, PR = prevalence rate (per 1,000 population)
Table 2: Socio-demographic characteristics of admission
malaria in Si Sa Ket province
|
Characteristics
|
Normal malaria cases (%)
|
Severe malaria cases
(%)
|
P-value
|
|
Sex
Female
Male
|
64 (36.8)
331 (26.3)
|
110 (63.2)
926 (73.67)
|
<0.01
|
|
Age group (years)
Newborn to 15-year-old
16- to 45-year-old
More than 45-year-old
|
19 (26.8)
254 (27.1)
122 (28.8)
|
52 (73.24)
682 (72.9)
302 (71.2)
|
0.825
|
|
Occupation
Student
Farmer
Government officer
Military personnel
Other
|
21 (23.6)
211 (30.6)
47 (35.6)
24 (10.6)
92 (31.3)
|
68 (76.4)
478 (69.4)
85 (64.4)
203 (89.4)
202 (68.7)
|
<0.000
|
|
Nationality
Thai
Foreigner
|
388 (27.8)
7 (19.4)
|
1,007 (72.2)
29 (80.6)
|
0.347
|
|
Malaria species
Pf
Pv
Mixed and other
|
101 (25)
134 (21.9)
53 (41.7)
|
303 (75)
479 (78.1)
74 (58.3)
|
<0.000
|
Pf = Plasmodium.falciparum, Pv = Plasmodium vivax, Mixed =
Mixed of Plasmodium falciparumandPlasmodium vivaxorPlasmodium
malariea;p-value significant at < 0.05
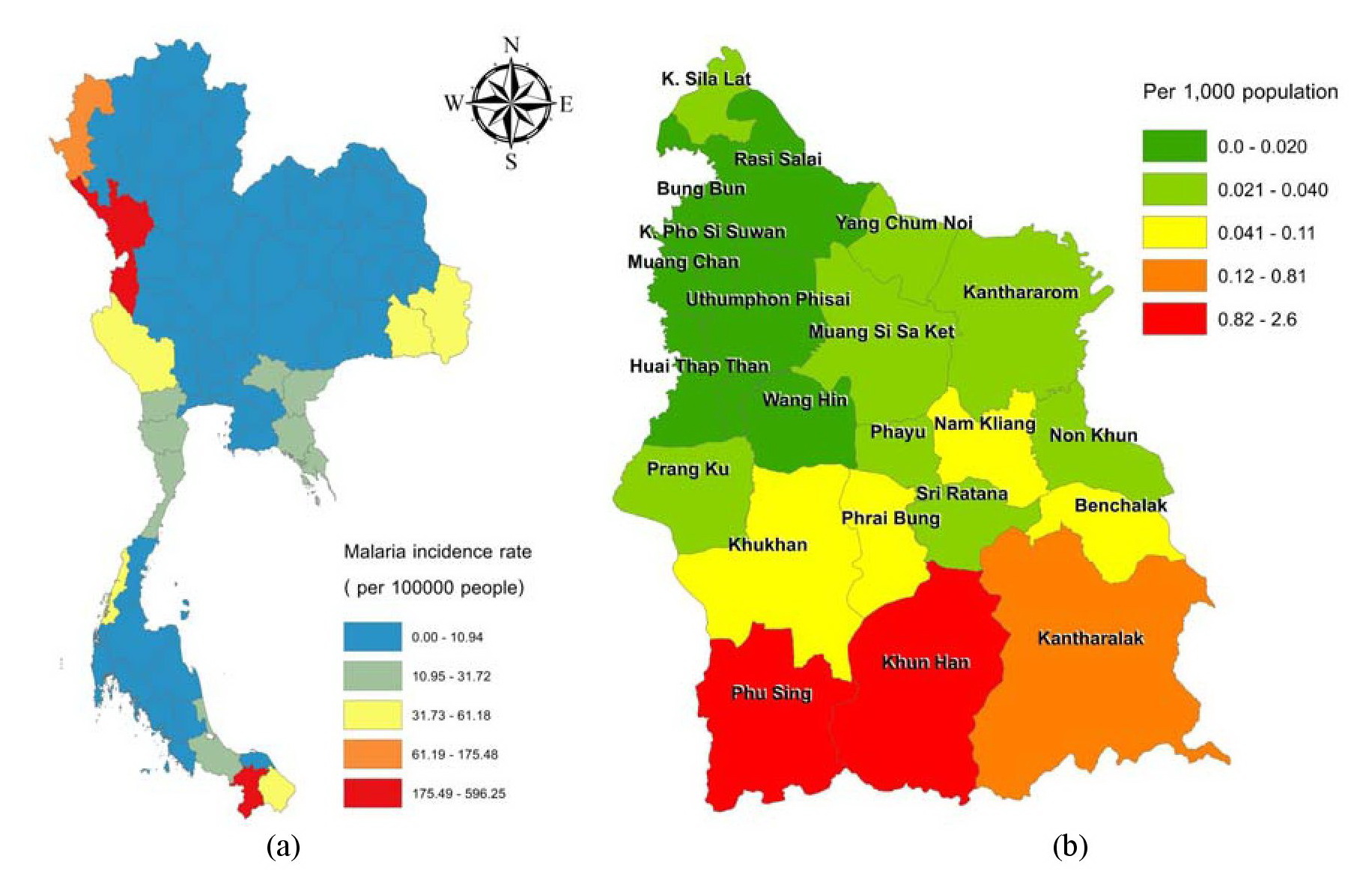
Figure 2: Study area and the overall incidence during
2015 to 2020 (a) Thailand map (b) Si Sa Ket map
In general, malaria is a seasonal epidemic. It slightly increases
starting from the rainy season starting from week 18. The peak of the
malaria season was found to be May to June and October. Table 2 shows
no factors related to severe malaria, age (P-value = 0.825) and
nationality (P-value = 0.347). The factors related to severe malaria
are sex (P-value < 0.01), occupation (P-value<0.001) and malaria
species (P-value<0.001).
3.2 Geographical Malaria Distribution in Si Sa Ket Province
Malaria in Thailand, It’s still high along border areas such as
Thai-Myanmar, Thai-Malaysia, and Thai-Cambodia, especially Thai-Myanmar
(Figure 2). Moreover, the Thai-Cambodia border remains antimalarial
drug-resistant. In Si Sa Ket situation, the districts with high levels
of malaria phenomenon were along the national border (Thai -Cambodia)
in the southern section, such as at Khun Han, Phu Sing and Kantharalak.
Most districts had a low incidence of malaria. People's movements were
a significant problem affecting the incidence of malaria. People in
low-endemic areas travelled to regions with high malaria incidence
because of occupational demands, bringing malaria back to their homes.
Therefore, malaria spreads in every district of Si Sa Ket province
(Figure 2). Figure 3 shows a decrease in the malaria incidence during
the last two years in 2019 and 2020. We also investigated are related
to the distribution of malaria, population density, and factors. Figure
4 illustrates that malaria prevalence significantly decreased from 2015
to 2020, particularly in the southern part of the study area. From 2015
to 2018, malaria incidence was proportional to population density;
however, after 2018, the correlation no longer exists because of lower
malaria infection rate after 2018 as shown in Figure 5. Altitude is
another factor that affects the malaria infection rate. Figure 6
demonstrates that the higher the elevation, the lower the malaria
infection rate.
3.3 Risk Factors of Severe Malaria Cases in Si Sa Ket Province
Table 2 shows factors related to severe malaria. There was no
statistically significant age (p-value = 0.825) and nationality
(P-value = 0.347). In the univariable analysis, we found that some
variables are influenced to severe malaria, male (P-value < 0.01,
95% Confidence interval (CI) = 1.17 - 2.27), occupation: military
personnel (P-value < 0.01, 95% Confidence interval (CI) = 1.37 -
4.99) and malaria type: Mixed (P-value < 0.001, 95% Confidence
interval (CI) = 0.3 - 0.71). And then, they added all the variables into
a multivariable logistic regression analysis for a robust model. We
found that the male sex was more chance of severe malaria than the
female: 2.49x (P-value = 0.013, Adjust Odds Ratio (AOR) = 2.49; 95%CI =
1.11-2.45).
Military personnel were 2.93x (P-value <0.01, Adjust Odds Ratio
(AOR) = 2.93; 95%CI = 1.45-6.57) more likely to be severe malaria than
students. Plasmodium falciparum had lower odds of being the
causative agent of malaria in a severe malaria case than Mixed and
others (P-value < 0.01, Adjust Odds Ratio (AOR) = 3.34, 95%CI =
0.31-0.73) (Table 3).
3.4 Environment Variables and Malaria Incidence
In addition to environmental factors, meteorological factors were
associated with malaria incidence in the province. Table 4 shows that
malaria incidence was negatively related to population density with no
statistical significance (P-value > 0.05).
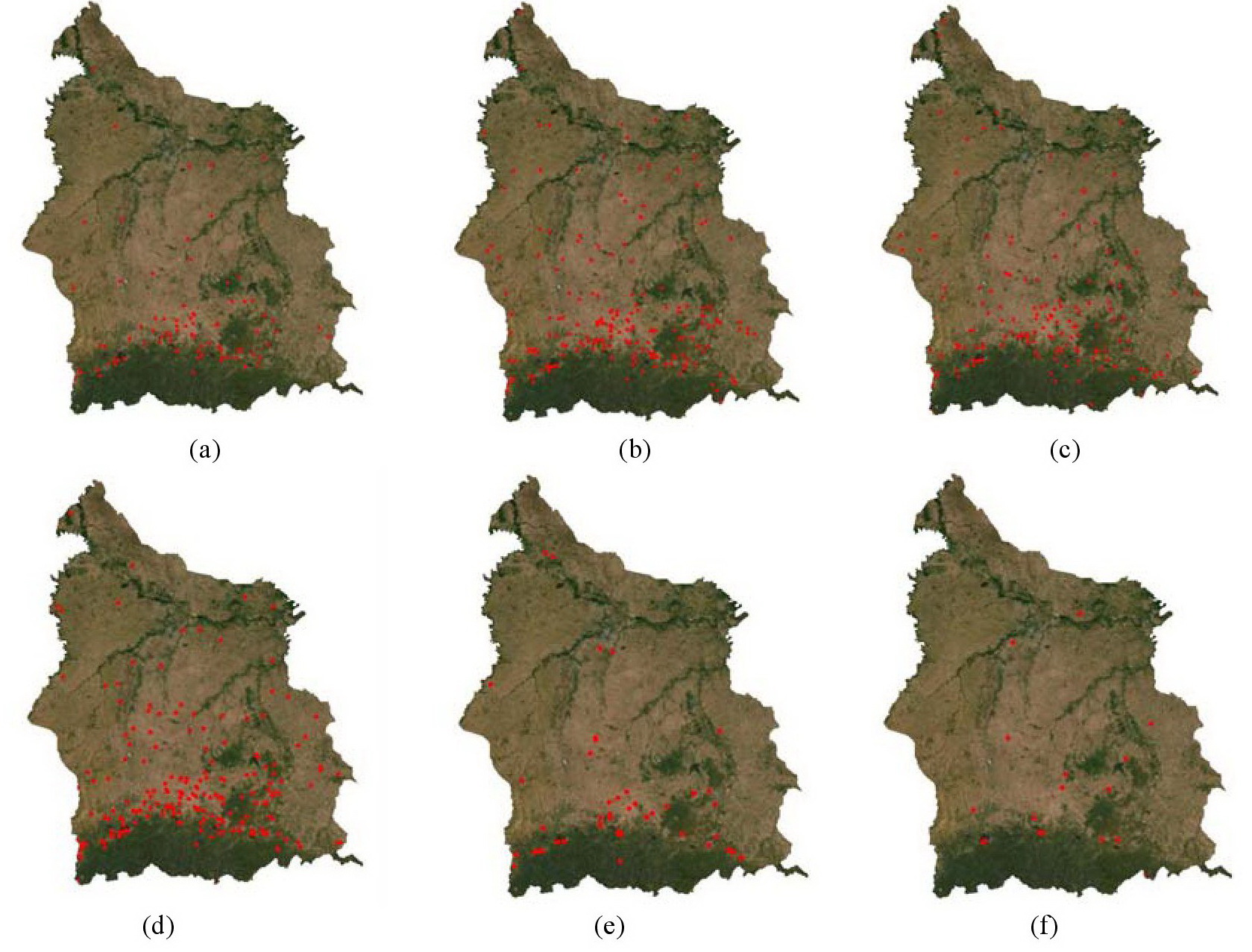
Figure 3: The malaria distribution in Si Sa Ket
Province (a) 2015, (b) 2016, (c) 2017, (d) 2018 (e) 2019, (f) 2020
Table 3: Factors related to severe malaria cases in Si
Sa Ket province
|
Characteristics
|
Univariable
|
Multivariable
|
|
OR (95%CI)
|
P value
|
AOR (95%CI)
|
P value
|
|
Sex
Female
Male
|
Ref.
2.87 (1.17 - 2.27)
|
<0.01
|
Ref.
2.49 (1.11 - 2.45)
|
0.013
|
|
Occupation
Student
Farmer
Government officer
Military personnel
Other
|
Ref.
1.36 (0.42 - 1.17)
1.89 (0.3 - 1.02)
2.91 (1.37 - 4.99)
1.39 (0.39 - 1.17)
|
0.174
0.059
<0.01
0.165
|
Ref.
0.92 (0.41 - 1.38)
1.2 (0.32 - 1.32)
2.93 (1.45 - 6.57)
0.89 (0.39 - 1.42)
|
0.357
0.232
<0.01
0.373
|
|
Species
Pf
Pv
Mixed and other
|
Ref.
1.16 (0.89 - 1.6)
3.58 (0.3 - 0.71)
|
0.245
<0.001
|
Ref.
1.21 (0.89 - 1.64)
3.34 (0.31 - 0.73)
|
0.225
<0.01
|
OR = Odd ratio; AOR = Adjust Odd ratio; Ref. = reference;
Pf = Plasmodium falciparum, Pv = Plasmodium vivax
, Mixed = Mixed of Plasmodium falciparumandPlasmodium
vivaxorPlasmodium malariea;p-value significant
at < 0.05
Table 4: Spearman rank correlation of malaria cases and
other ecological factors at Si Sa Ket, Thailand
|
Factors
|
Observe
|
Correlation
|
P-value
|
|
Average temperature
|
60
|
0.0064
|
0.961
|
|
Average rainfall
|
60
|
0.1284
|
0.328
|
|
Population density
|
60
|
-0.15
|
0.506
|
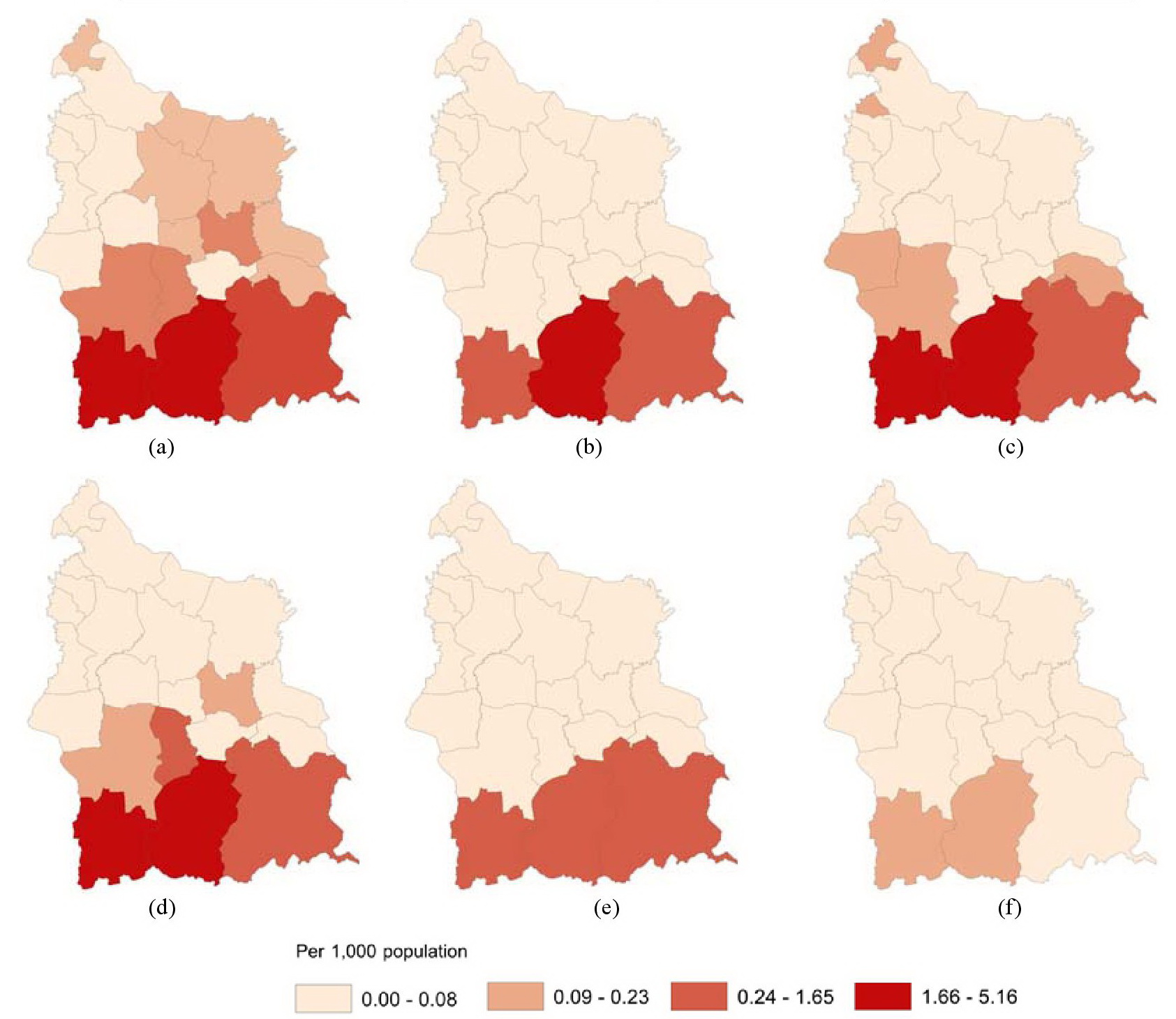
Figure 4: Malaria prevalence in Si Sa Ket province (a)
2015, (b) 2016, (c) 2017, (d) 2018, (e)2019, (f) 2020
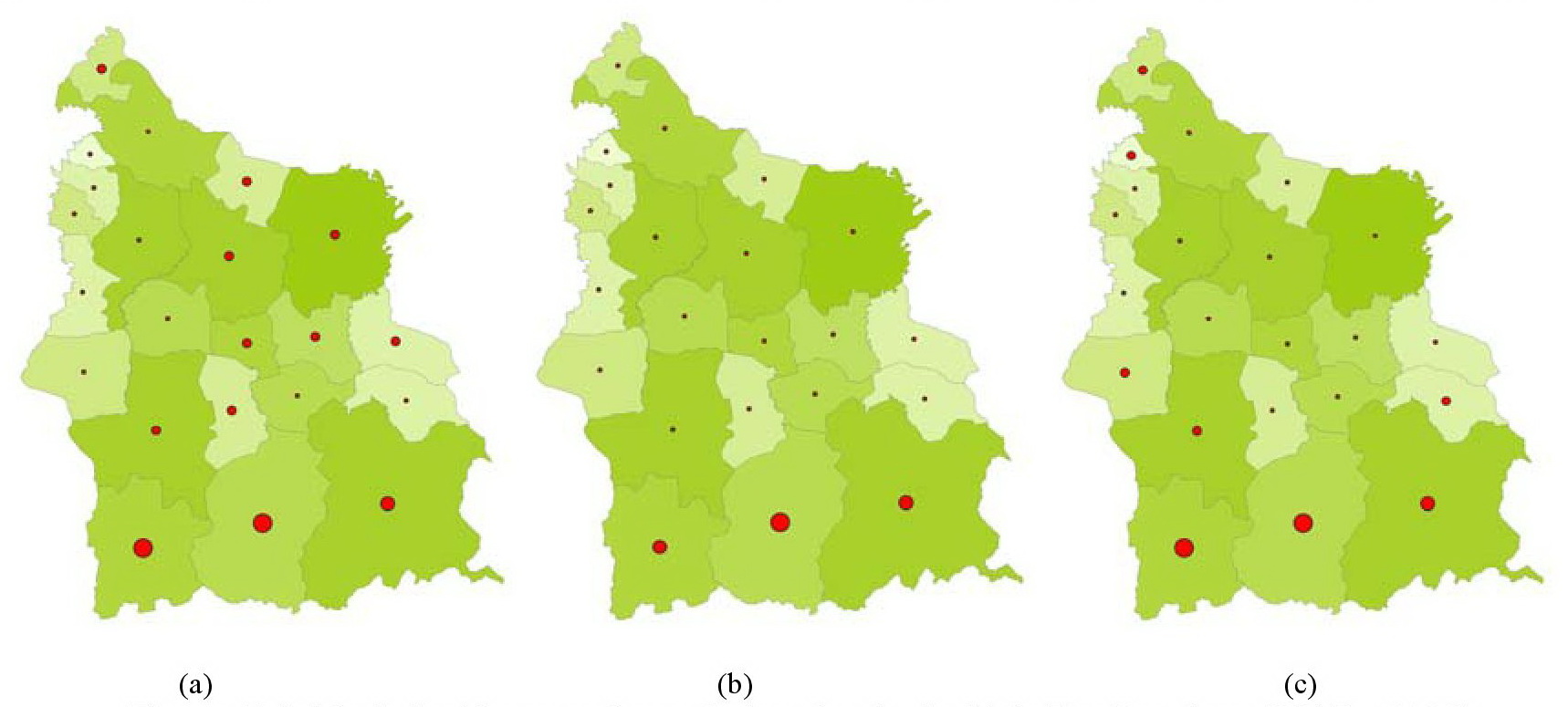
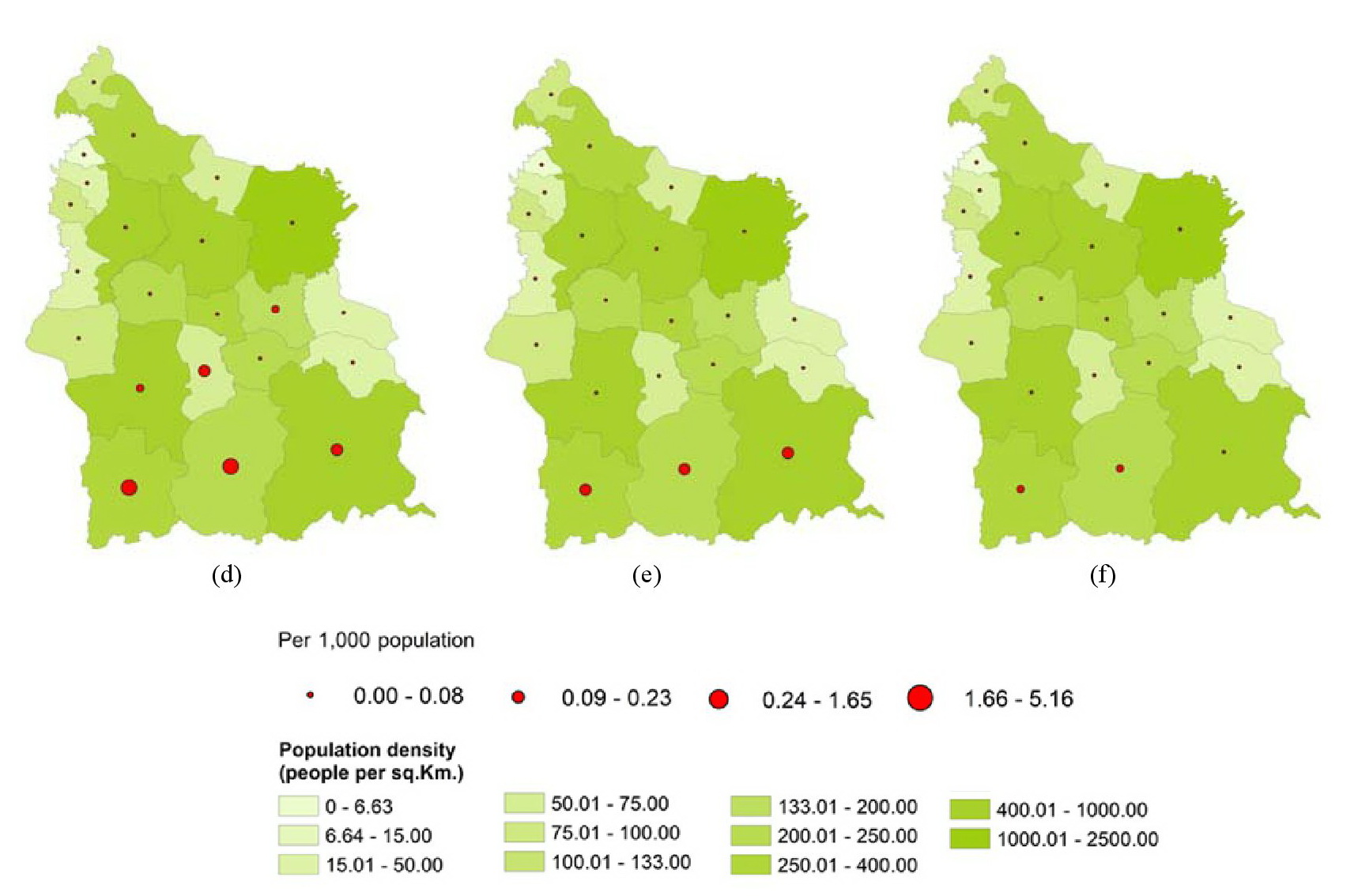
Figure 5: Malaria incidence and population density in
Si Sa Ket Province (2015 – 2020)
(a) 2015, (b) 2016, (c) 2017, (d) 2018, (e) 2019, (f) 2020
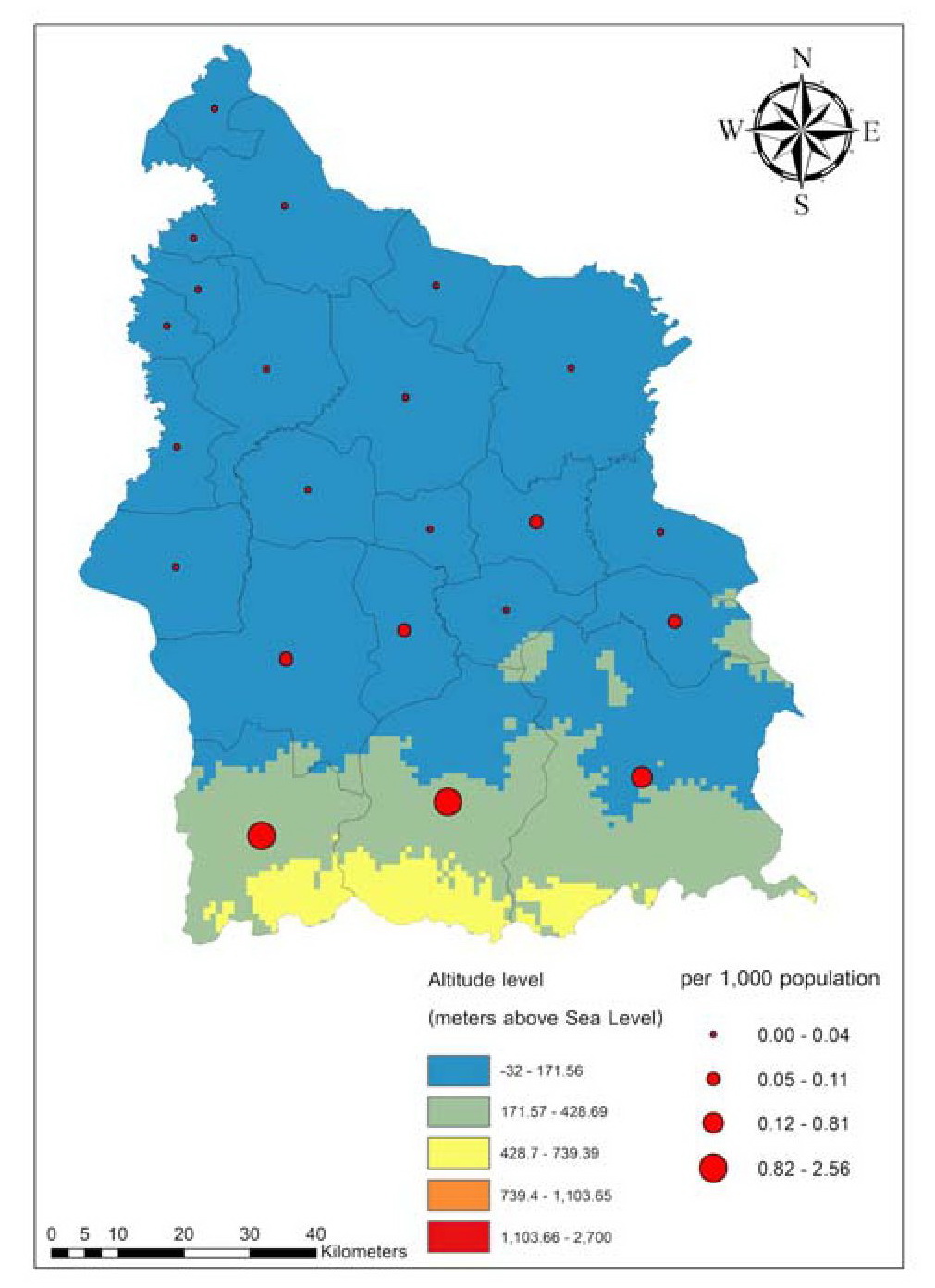
Figure 6: Average malaria incidence during 2015 - 2020
and altitude in Si Sa Ket province
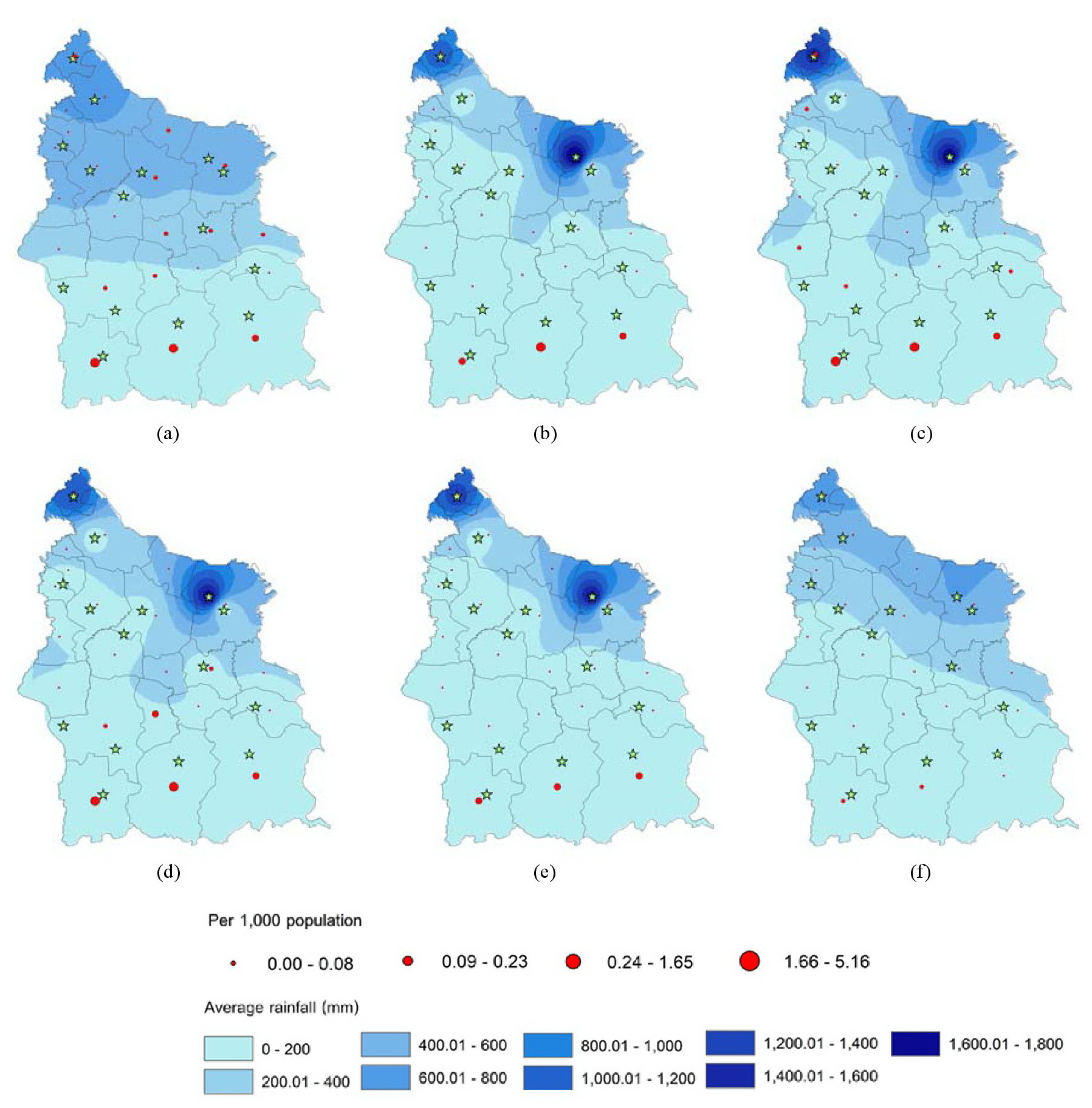
Figure 7: The average rainfall per year and malaria
incidence in Si Sa Ket Province during 2015 – 2020 (a) 2015, (b) 2016, (c) 2017, (d) 2018, (e) 2019, (f) 2020
The average temperature was a mild positive relationship to malaria
incidence with no statistical significance (P-value > 0.05). Average
rainfall was a soft positive relationship to malaria incidence with no
statistical significance (P-value > 0.05) (Figure 7). Likewise,
water is a significant factor in the Anopheles mosquito's
reproduction. Generally, Anopheles mosquitoes prefer to lay
their eggs in highland, densely forested areas with slow-flowing water
(Figure 7).
4. Discussion and Conclusion
This report combines spatial and climatic data to describe malaria
trends and epidemiology in Si Sa Ket province from 2015 to 2020.
Moreover, create and generate a spatial environmental map of malaria
incidence. Our crucial findings showed that malaria has decreased over
the entire study period. The average annual incidence of malaria
reported in Si Sa Ket province was 0.47 per 1000 population between
2015 to 2020. It dramatically decreased from 2018 to 2020. “World
Malaria Day 2018”, Thailand recognizes 35 malaria-free provinces.
Furthermore, The Ministry of Public Health emphasizes that participation
from local agencies is critical to eliminating malaria [13]. Factors
are related to the admission of malaria cases. This study describes
that >70% of malaria cases were male. Military personnel had more
chance of being admitted with severe malaria than other occupations.
Border across.
It is a significant problem in the spread of malaria. There are reports
of studies on population movement. That is related to malaria
concentration. For some reason, humans can be a reservoir host for
malaria [27] and [28]. Malaria screening and control units in
partnership with related corporations like the Military should be
undertaken [29]. A type of malaria can be related to severe malaria.
This study shows the odds of severe in patients with more than one
malaria species. In contrast, the study of Wangdi and Lon found that
the most severe malaria will be P. falciparum [30] and [31].
The hotspots of indigenous malaria were in the southern part of Si Sa
Ket province. This part of Si Sa Ket province is a forest area and
national border. The main occupation is agriculture. Thus, patients
with severe malaria were military personnel. These groups are at a
higher risk for malaria disease [32]. Environmental factors such as
temperature are crucial in a malaria transmission cycle and mosquito
survival [33] and [34]. This study found that average temperature and
average rainfall had a mild positive relationship with malaria but no
statistical significance. Likewise, some studies have explained rainfall
as a crucial factor in malaria transmission [35] and [36].
Temperature < 16 °C had detrimental effects on mosquito endurance,
and temperature also decreased with increasing altitude [37] and [38].
This study found that areas at higher altitudes had a high burden of
malaria. In conclusion, malaria remains a public health problem. The
outcome of this research can be supported by a malaria monitoring
system. This study indicated that health agencies are achieving
relative success. Because malaria rates were lower than in other
studies. We hope to provide helpful info to local and Si Sa Ket
Province stakeholders to expand malaria prevention programs or mobile
applications for malaria combat. Moreover, Geographic information
system applications remain a crucial tool for disease control.
Acknowledgement
The authors greatly appreciate the grant from Research Affairs
Division, Faculty of Medicine, Mahasarakham University. Our thanks are
also extended to the General Communicable Disease Control Division, Si
Sa Ket Provincial Health Office, Si Sa Ket Province, Thailand, for the
malaria data and their generous assistance in carrying out this project
to the volunteers of those villages.
Reference
[1] Wongpituk, K., Kalayanarooj, S. and Nithikathkul, C., (2020).
Geospatial Analysis of DHF Surveillance Model in Si Sa Ket Province,
Thailand using Geographic Information System.
International Journal of Geoinformatics,
Vol. 16(3). 97-104.
[2] Toemjai, T., Thongkrajai, P. and Nithikathkul, C., (2022).
Factors Affecting Preventive Behaviour Against Leptospirosis among the
Population at Risk in Si Sa Ket, Thailand. One Health,Vol. 14.
https://doi.org/10.1016/j.onehlt.2022.100399.
[3] Thessingha, C., Wongsawad, C., Homchampa, P., Laothiang, P. and
Nithikathkul. C., (2019). Soil-Transmitted Helminthiases and Risk
Factors among Thai Hill-Tribe Preschool-Age Children in Remote Area of
Thailand. Journal of the Medical Association of Thailand.Vol.
102(8), 56-62.
[4] Soncharoen, P., Jongthawin, J. and Nithikathkul, C., (2022).
Influent Factor Toward Based Helminth Infections among of
Thai-Cambodian Border in Phusing District, Sisaket Province, Thailand.
International Journal of Geoinformatics.Vol. 18(5).
https://doi.org/10.52939/ijg.v18i5.2375.
[5] Nithikathkul, C., Wongsaroj, T., Buntilov, V. and Limsomboon,
J., (2012). Geographic Information System of Fish-Borne Parasitic
Zoonoses Metacercaria from Water Reservoirs under his Majesty's
Recommended Project, Phitsanulok, Thailand.
International Journal of Geoinformatics.
Vol. 8(3), 53-57.
[6] Nithikathkul, C., Trevanich, A., Wongsaroj, T., Wongsawad, C.
and Reungsang P., (2017). Health Informatics Model for Helminthiasis in
Thailand. Journal of Helminthology.Vol. 91(5).
https://doi.org/10.1017/S0022149X16000614.
[7] Kanjaras, P., Bumrerraj, S., Seng, R., Noradee, S. and
Nithikathkul, C., (2023). Geospatial Analysis and Modeling of
Melioidosis Prevention and Control in Si Sa Ket Province, Thailand.
International Journal of Geoinformatics.Vol. 19(1), 57–65,
https://doi.org/10.52939/ijg.v19i1.2501.
[8] Buntilov, V., Wattanayingcharoenchai, S., Nithikathkul, C. and
Wongsaroj, T., (2011). A Geographic Information System for Estimating
the Prevalence of Helminthiasis Infections in the North-Eastern
Thailand.
32nd Asian Conference on Remote Sensing 2011, ACRS 2011
. Vol. 2, 1170-1175.
[9] Nithikathkul, C., Reungsang, P., Trivanich, A., Homchumpa, P.,
Tongsiri, S. and Wongsawad, C., (2014). Geographic Information of
Fish-Borne Parasitic Metacercaria in Chi River, Mahasarakham, Thailand.
International Journal of Geoinformatics.Vol. 10(1), 25-29.
[10] Center of Disease Control and Prevention, (2018). CDC - Parasites –
Malaria. [Online]. Available:
https://www.cdc.gov/parasites/malaria/index.html.
[11] Kachur, S. P., (2022). Malaria.
Maxcy-Rosenau-Last Public Health & Preventive Medicine, 16e
, Boulton M.L. and R.B. Wallace Eds. New York: McGraw Hill.
[12] World Health Organization, World Malaria Report, (2018). Switzerland:
World Health Organization, 2018.
[13] World Health Organization, (2018).
Countries of the Greater Mekong are Stepping up to End Malaria
. Switzerland.
[14] Imwong, M., Suwannasin, K., Kunasol, C., Sutawong, K., Mayxay, M.,
Rekol, H., Smithuis, F. M., Hlaing, T. M., Tun, K. M., van der Pluijm, R.
W., Tripura, R., Miotto, O., Menard, D., Dhorda, M., Day, N. P. J., White,
N. J. and Dondorp, A. M., (2017). The Spread of Artemisinin-Resistant
Plasmodium falciparum
in the Greater Mekong Subregion: A Molecular Epidemiology Observational
Study. The Lancet Infectious Diseases.Vol. 17(5). 491-497.
https://doi.org/10.1016/S1473-3099(17)30048-8.
[15] Phyo, A. P., Nkhoma, S., Stepniewska, K., Ashley, E. A., Nair, S.,
McGready, R., ler Moo, C., Al-Saai, S., Dondorp, A. M., Lwin, K. M.,
Singhasivanon, P., Day, N. P. J., White, N. J., Anderson, T. J. C. and
Nosten, F., (2012). Emergence of Artemisinin-Resistant Malaria on the
Western Border of Thailand: A Longitudinal Study. The Lancet.Vol.
379, 1960-1966.
https://doi.org/10.1016/S0140-6736(12)60484-X.
[16] Ministry of Public Health, (2018). National Malaria Elimination
Strategy, Thailand 2017 – 2026. Nonthaburi, Thailand.
[17] Paaijmans, K. P., Blanford, S., Bell, A. S., Blanford, J. I., Read,
A. F. and Thomas, M. B., (2010). Influence of Climate on Malaria
Transmission Depends on Daily Temperature Variation.
Proc. Nat. Acad. Sci. USA
, Vol. 107(34), 15135-15139.
https://doi.org/10.1073/pnas.1006422107.
[18] The Open University, (2022, December 22). Study Session 6 Factors
that Affect Malaria Transmission. [Online]. Available:
https://www.open.edu/openlearncreate/mod/oucontent/view.php?id=89&printable=1.
[19] Jean, P., (1992). Animal Production in the Tropical. Basing Stoke,
UK: MacMillan.
[20] Dlamini, S. N., Franke, J. and Vounatsou, P., (2015). Assessing the
Relationship between Environmental Factors and Malaria Vector Breeding
Sites in Swaziland using Multi-Scale Remotely Sensed Data.
Geospatial Health,
Vol. 10(1).
https://doi.org/10.4081/gh.2015.302.
[21] Department of Provincial Administration, (2020). Registry Statistic
System. [Online]. Available:
http://stat.dopa.go.th/stat/statnew/statMenu/newStat/home.php.
[22] Climatedata.org, (2020). Climate Si Sa Ket 2015 - 2020. [Online].
Available:
http://en.climate-data.org/saia/thailand/Si-Sa-Ket-Province/Si-Sa-Ket-37437/".
[23] Wayant, N. M., Maldonado, D., Rojas de Arias, A., Cousiño, B. and
Goodin, D. G., (2010). Correlation between Normalized Difference Vegetation
Index and Malaria in a Subtropical Rain Forest Undergoing Rapid
Anthropogenic Alteration. Geospat Health,Vol. 4(2).
https://doi.org/10.4081/gh.2010.199.
[24] Center of Disease Control and Prevention, (2018). Malaria Diagnostic
Tests. [Online]. CDC. Available:
https://www.cdc.gov/malaria/diagnosis_treatment/diagnostic_tools.html.
[25] DIVA-GIS, (2020). Thailand boundary. [Online]. Available:
https://data.biogeo.ucdavis.edu/data/diva/adm/THA_adm.zip.
[26] Northeastern Meteorological Center, (2020). Meteorological and
Environmental Data on Si Sa Ket Province 2015 – 2020. Ubonratchathani,
Thailand: Thai Meteorological Department.
[27] Saita, S., Silawan, T., Parker, D. M., Sriwichai, P., Phuanukoonnon,
S., Sudathip, P., Maude, R. J., White, L. J. and Pan-ngum, W., (2019).
Spatial Heterogeneity and Temporal Trends in Malaria on the Thai–Myanmar
Border (2012–2017): A Retrospective Observational Study.
Tropical Medicine and Infectious Disease,
Vol. 4(2). Available:
https://www.mdpi.com/2414-6366/4/2/62.
[28] Bhumiratana, A., Intarapuk, A., Sorosjinda-Nunthawarasilp, P.,
Maneekan, P. and Koyadun, S., (2013). Border Malaria Associated with
Multidrug Resistance on Thailand-Myanmar and Thailand-Cambodia Borders:
Transmission Dynamic, Vulnerability, and Surveillance.
BioMed Research International.
Vol. 2013.
https://doi.org/10.1155/2013/363417.
[29] Fahmi, F., Pasaribu, A. P., Theodora, M. and Wangdi, K., (2022).
Spatial Analysis to Evaluate Risk of Malaria in Northern Sumatera,
Indonesia. Malaria Journal,Vol. 21(1).
https://doi.org/10.1186/s12936-022-04262-y.
[30] Wangdi, K., Furuya-Kanamori, L., Clark, J., Barendregt, J. J.,
Gatton, M. L., Banwell, C., Kelly, G. C., Doi, S. A. R. and Clements, A. C.
A., (2018). Analysis of Clinical Malaria Disease Patterns and Trends in
Vietnam 2009–2015. Malaria Journal,Vol. 17(1).
https://doi.org/10.1186/s12936-018-2478-z.
[31] Lon, C., Timmermans, A., Buathong, N., Nou, S., Se, Y., Sitthy, N.,
Chann, S., Kraesub, S., Wongstitwilairoong, T., Walsh, D. S., Tyner, S.,
Fukuda, M., Callender, D., Sherwood, J., Koy, L., Char, M., Bethell, D. and
Saunders, D., (2013). Severe Malaria in Battambang Referral Hospital, an
Area of Multidrug Resistance in Western-Cambodia: A Retrospective Analysis
of Cases from 2006–2009. Malaria Journal,Vol. 12(1).
https://doi.org/10.1186/1475-2875-12-217.
[32] Herdiana, H., Cotter, C., Coutrier, F. N., Zarlinda, I., Zelman B.
W., Tirta, Y. K., Greenhouse, B., Gosling, R. D., Baker, P., Whittaker, M.
and Hsiang, M. S., (2016). Malaria Risk Factor Assessment Using Active and
Passive Surveillance Data from Aceh Besar, Indonesia, a Low Endemic,
Malaria Elimination Setting with Plasmodium Knowlesi, Plasmodium vivax, and
Plasmodium Falciparum. Malaria Journal,Vol. 15(1).
https://doi.org/10.1186/s12936-016-1523-z.
[33] Noden, B. H., Kent, M. D. and Beier, J. C., (1995). The Impact of
Variations in Temperature on Early Plasmodium falciparum Development in
Anopheles stephensi. Parasitology,Vol. 111(5).
https://doi.org/10.1017/s0031182000077003.
[34] Brooker, S.,Clarke, S., Njagi, J. K., Polack, S., Mugo, B.,
Estambale, B., Muchiri, E., Magnussen, P. and Cox, J., (2004). Spatial
Clustering of Malaria and Associated Risk Factors During an Epidemic in a
Highland Area of Western Kenya.
Tropical Medicine & International Health,
Vol. 9(7).
https://doi.org/10.1111/j.1365-3156.2004.01272.x.
[35] Craig, M. H., Snow, R. W. and le Sueur, D., (1999). A Climate-based
Distribution Model of Malaria Transmission in Sub-Saharan Africa.
Parasitology Today,
Vol. 15(3).
https://doi.org/10.1016/S0169-4758(99)01396-4.
[36] Thomson, M. C., Mason, S. J., Phindela, T. and Connor, S. J., (2005).
Use of Rainfall and Sea Surface Temperature Monitoring for Malaria Early
Warning in Botswana. Am J Trop Med Hyg.,Vol. 73(1). 214-221.
[37] Sena, L., Deressa, W. and Ali, A., (2014). Dynamics of
Plasmodium falciparum
and Plasmodium vivax in a Micro-Ecological Setting, Southwest
Ethiopia: Effects of Altitude and Proximity to a Dam.
BMC Infectious Diseases.
Vol. 14(1).
https://doi.org/10.1186/s12879-014-0625-x.
[38] Woyessa, A., Deressa, W., Ali, A. and Lindtjørn, B., (2012).
Prevalence of Malaria Infection in Butajira Area, South-Central Ethiopia.
Malaria Journal,Vol. 11(1).
https://doi.org/10.1186/1475-2875-11-84.
